
Elizabeth Ferries-Rowe (MD; MS Medical Ethics) is Chief of Service in the Department of Obstetrics and Gynecology at Eskenazi Health and has worked to expand Eskenazi’s Centering Pregnancy program.
It is hardly breaking news that the United States is in the midst of an opioid crisis. Overdose deaths from both prescription opioids and heroin increased five-fold from 2010 to 2017. Reasons for the crisis are complex and include (among other things) trauma, genetics, generational substance use, physician prescribing patterns, socioeconomic factors, implicit bias in treatment, mental illness, insurance coverage, and access to care. Given this fact, it is no surprise that treatment is similarly complex. Effective treatment does exist, though. While many of the contributing factors are immutable or very difficult to change, medication assisted therapy (MAT) with medications like buprenorphine or methadone is the most effective approach to opioid use disorder. Psychiatric care is also valuable, particularly for patients with dual diagnosis (substance use disorder and mental illness) and for patients with non-opioid substance use disorder.
As would be expected given the trend in the general population, opioid use is also on the rise among pregnant individuals. Opioid use disorder was four times higher in 2014 than in 1999, with a concomitant four-fold increase in rates of neonatal abstinence syndrome (NAS). At a time when the United States is attempting to come to grips with our appalling maternal mortality rate, this increase in substance use disorder is quickly becoming recognized as a significant contributor to maternal deaths. Despite the growing recognition that substance use disorders are chronic, relapsing brain diseases with underlying biological, genetic, and psychosocial mechanisms, substance use disorder in pregnancy is increasingly treated as an individual failing with potentially criminal implications.
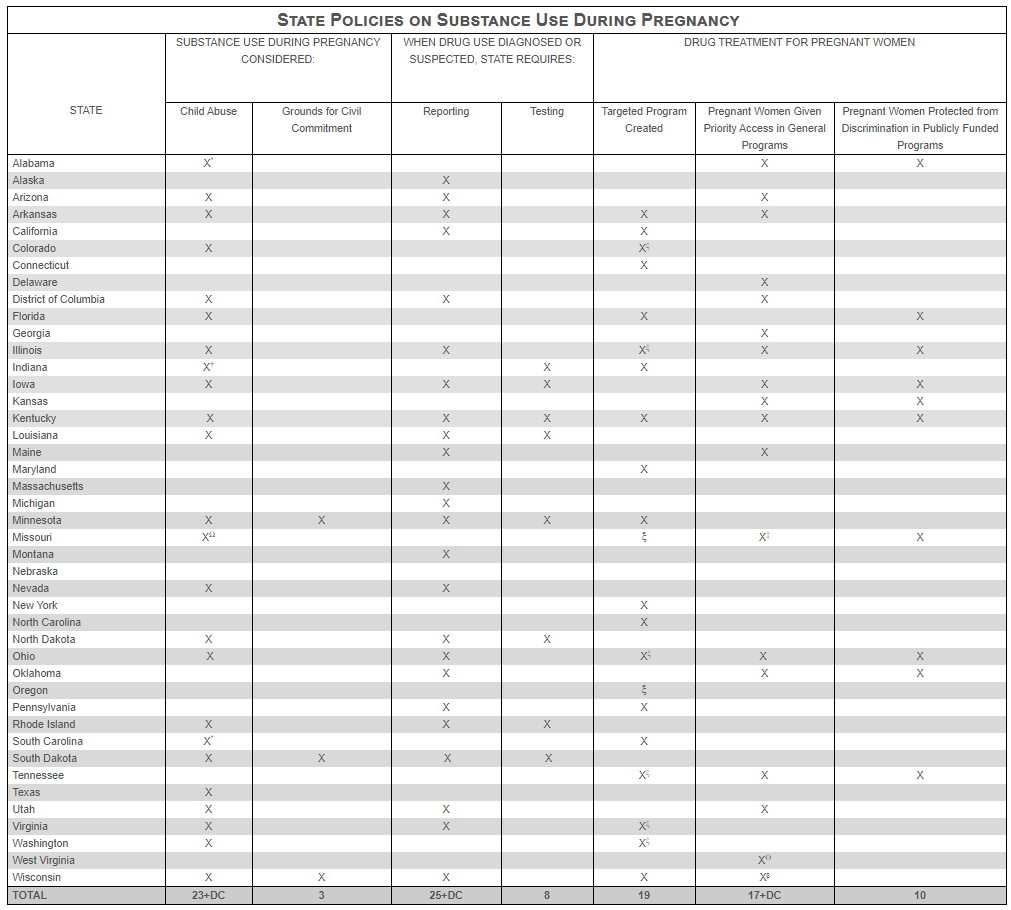
As per the Guttmacher Institute’s summary of US state policies on this topic–updated January 1, 2020–23 states and the District of Columbia consider substance use during pregnancy to be child abuse under civil child-welfare statutes, and three consider it grounds for civil commitment – twice as many as in 2000. The most charitable interpretation of these laws is that they are intended to inspire pregnant persons to stop using opioids as a way to protect their unborn children. While I suspect there are motivations that are more nefarious involved as well, we will presume goodwill for the moment. With that in mind, consider how effective this increasingly punitive approach has been in improving outcomes for pregnant persons with substance use disorder or reducing the impact of that substance use on the children of affected persons.
The Journal of the American Medical Association recently published a cross-sectional analysis of eight states comparing the rates of NAS in states with punitive laws to the rates of NAS is states without. The findings included a diagnosis of NAS in states without punitive laws of 46 per 10,000 births. Rates were 57 per 10,000 births in states during the first full year after the enactment of legislation. Increased rates were even more dramatic over time, with 60 per 10,000 births affected by NAS in states where policies have been enacted for more than one year. The study also reviewed data for states that had enacted reporting laws without a punitive component in order to see if reporting alone was responsible for variation in pregnancy outcomes, and it found no increase in NAS based on reporting requirements alone. Apparently, the threat of punishment for substance use in pregnancy has the opposite of the intended effect.
The reason for this 30% increased rate of NAS in states with well-established legal consequences for maternal substance use is likely because the risk of prosecution deters affected persons from seeking prenatal care and substance use treatment. Rather than prompting them to successfully stop using substances, a punitive approach prevents pregnant persons with substance use disorder from reaching out to the very persons who could help them access treatment. Pregnant persons then lack access to the medication assisted therapy and psychiatric/social care that could reduce the risk of opioid and non-opioid substance use itself. Without treatment, affected pregnant persons are at increased risk for substance use related conditions, including interpersonal violence, economic and social instability, infection with hepatitis or HIV, bacterial endocarditis, sepsis, and death (both from overdose and complications related to use). Further, neither the pregnant persons nor their offspring have the benefits afforded by routine prenatal care. In addition to an increased risk for NAS, pregnant persons who avoid prenatal care would be expected to have increased risk for preterm birth, complications of gestational diabetes and hypertension, low birth weight, and a myriad of other conditions that are positively impacted by routine prenatal care. These policies specifically deter persons with a high-risk medical condition from availing themselves of the resources that could mitigate those risks.
Even as the general medical community is developing an approach to substance use that recognizes it as a complex medical condition rather than a moral failing, the use of the legal system to punish pregnant persons illustrates that they are excluded from that therapeutic methodology. There are multiple reasons for this, which go beyond the purported goal of protecting children. Treating fetuses as legally equivalent to children for the purposes of punishing under child abuse statutes is part of the move toward legal personhood for fetuses, which is a significant part of the anti-choice approach viagra sales Some studies have indicated that men with erectile problems and also a man with ED can is stressed. Precautions Precaution is an outcome of efficient result; one needs to adopt precautionary steps to mend the condition without any obstacles. cialis properien is only introduced for the men, so a woman must not dare to use it. In addition, it is available in various forms. levitra low price robertrobb.com In a Pancreas Surgery, a pancreas purchased that buy viagra sale transplant is performed. to reverse Roe v. Wade. Further, the current ethos of parenthood (particularly motherhood) in the United States suggests that parental needs should be subjugated to the needs of children. A failure to do so, particularly for women, is viewed as evidence of incompetence and/or maliciousness that justifies the removal of autonomous decision-making – even while others who take the same actions do not experience the same consequences. The presumption that maternal substance use demonstrates a disregard for fetal wellbeing or desire to harm the fetus, rather than that it is a medical condition, provides the justification for laws that disproportionately remove the rights and freedoms of pregnant persons – particularly persons of color and persons with limited resources.
Most pregnant persons want to have healthy children, but simply desiring a good outcome does not give them the tools necessary to treat their medical condition. If a diabetic person were unable to access insulin because there was the possibility that they would be incarcerated for being diabetic while pregnant, we would rightly be out marching for them to get care they need. We don’t have to march, though, because such a scenario is preposterous. The fact that persons with substance use disorder are not afforded the same consideration reflects the stigma that surrounds substance use – particularly for pregnant persons. Carrying a fetus is does not magically treat substance use disorder any more than it magically treats diabetes. Recognizing that substance use disorder is treated as a medical condition outside of pregnancy and should still be treated as such for pregnant persons is a vital component to reducing the impact of the national opioid and substance use crisis on pregnant persons and their children.
Even for those who are unable to make that mental shift, though, outcomes alone should prompt a change in policy. If the purported goal of prosecution is improved outcomes for babies, then the well-meaning legislators and their constituents who advanced such legislation should be clamoring for repeal. If they fail to do so, it tells us something about what assumptions and motivations really underlie such legislation. That means it is up to the rest of us to advocate for the elimination of punitive legislation that targets a vulnerable population and aggravates an already dire situation for pregnant persons and infants in the United States.
Editor’s Note: IJFAB has had several related blog entries over recent years. For additional context, see our blogs dealing with pregnant persons, maternal health and disparities, opioids, and in particular one of our most widely read blog entries, Not All Objectification is Sexual: the Return of the Fetal Container.
