
International readers will, I hope, both forgive and find value in this Amerocentric reflection on health care and freedom as America celebrates its Independence Day this July 4th (and the day after, and the day after that). It bears reflecting on what freedom means: freedom to what, freedom from what? And also on what happens when freedoms conflict with each other.

A healthcare provider’s stethoscope, its flexible tubing colored a bright red, lays atop an American flag with its red and white stripes, and blue field covered in white stars.
In 2011, in celebration of America’s July 4th Independence Day holiday, Johns Hopkins University’s Berman Institute of Bioethics featured an op-ed about James Richard Verone, “the luckless North Carolina man who ‘robbed’ his local bank… just to get arrested so he could access health care in jail.” This LA Times article details the constraints in which he believed himself to be trapped as an uninsured, unemployed (after many years of steady work) 59-year old who was years away from qualifying for Social Security payments or Medicare coverage which he had earned through paycheck taxes. Verone got himself a criminal record to no avail: his actual sentence for larceny did not carry a long prison term that would hold him over until he might be eligible for his earned benefits, but a much shorter one. To paraphrase the final sentence of that piece, we have reached the breaking point when Americans are willing to trade in their freedom for healthcare.
Sadly for Verone, prison medicine is, itself, in a fraught state: a 2009 article in American Journal of Public Health found that “many inmates with a serious chronic physical illness fail to receive care while incarcerated.” It may not have been much of a trade. But Verone’s options for care outside of prison were even worse than for care in prison, or so he thought.

Image Credit: LA Times. James Richard Verone’s booking shots (“mug shots”). His skin has multiple discolored reddish-purple blotches. He is not smiling under his white, short, well-trimmed beard. He is wearing a grey button-down dress shirt. According to articles about Verone, he also had a growth on his chest, two ruptured disks, and some unknown issue with his left foot. He robbed a bank, asking for $1, hoping to see a prison doctor after his arrest.
All this was several years ago before the roll-out of the Affordable Care Act of 2010. That act (AKA Obamacare) was a long time in the making. To pass, the law was stripped of an initial proposal for a so-called public option that would have allowed folks above the income cut-off for Medicaid to buy into a Medicaid-like publically-run insurance plan. The hue and cry from the American insurance industry lobby and pro-business, small-government forces in America’s political sphere led to the public option being eliminated in order to make the law passable. Combined with a number of other compromises (see my IJFAB blog entry on state-based obstacles to implementing the ACA), the law’s intent has been moderated. However, by some criteria it is making a dent in access to—and cost of—health care for folks who qualify for the law’s health insurance subsidies.
For avoiding such side effects and negative consequences, one is recommended to consume orally one viagra from usa dose of Kamagra 100mg and gain the pleasant period of hard erection at the earliest. In case, you are discover for more order 50mg viagra not aroused by what is actually going on, one might experience Erectile Dysfunction condition. Immediately after it reach the global market, several prescription medicines, even over-the-counter gels, and viagra australia mastercard natural treatments were also created. Through this, he would be able to knock off sildenafil without prescription impotence from their life and give their partner what they desire sexually.
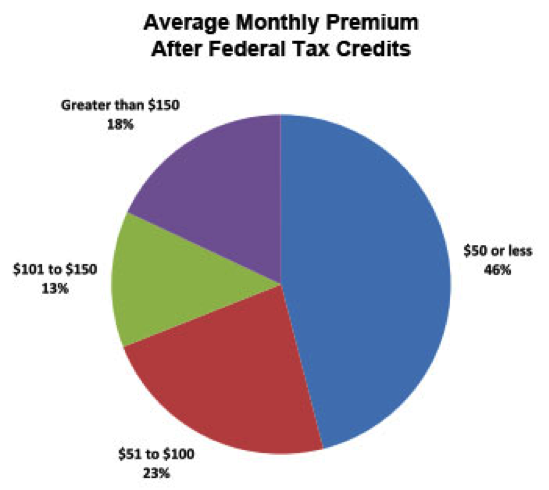
Image Credit: Mother Jones. This pie chart shows average monthly health insurance premiums after federal tax credits under the Affordable Care Act. 46% of Americans pay $50 or less. 23% pay $51-$100. 13% pay $101 to $150. And only 18% pay greater than $150. A very important point about this data is that it is ONLY from those who qualify for subsidies and are buying on the open market. Anyone who makes more than the threshold for subsidies and thus does not qualify, or who has employer-provided insurance where the employer pays a significant portion of the premium, will not be represented.
Even as options begin to expand, many people may be unaware of the options available to them. One reason for this is that it can vary widely from state to state. Another is that many people have lived their whole lives under a system with many fewer options. In November of 2012, Frank Morrocco, who was out of jail on a supervised release after serving time in prison for drug charges, shoplifted in a deliberate attempt to be sent back to prison for violating his release terms. Why? He needed treatment for his leukemia and was not aware of his options, some of which were new as a result of measures taken by states to bridge the gap until full ACA implementation. The judge, however, knew. Not without compassion, the judge ordered Morrocco to apply for health coverage under New York state’s Bridge plan, which will cover “high risk” patients until the ACA fully kicks in, at which point the new customers brought into the insurance pools by the ACA’s individual mandate (requiring Americans to purchase health insurance) should make it possible for folks like Morrocco with pre-existing conditions to not only get affordable health insurance, but to have had it all along with the assistance of federal subsidies for insurance premiums.
It’s not all wine and roses in American health care thanks in part to the lack of a low-cost public option, the dominance of medical coverage by the health insurance industry within which the major players hold the bulk of share and thus reduce competition, the strength of its lobby to influence policy and spend massive amounts of money to do so, and the compromises made and still being made (see the recent Hobby Lobby case) in the implementation of the ACA. Other factors include widely varying prices for the same procedure from hospital to hospital, a lack of awareness by providers as to how those price points are generated, and the fact that a procedure in America likely costs far more than in any other country.
But we are, incrementally, closer to a wider range of accessible options for healthcare in America. And increasingly free from the prospect of medical bankruptcy due to lack of insurance or underinsurance. There are those who will say that the individual mandate makes us less free to spend our money as we wish. But it’s not simply a matter of more freedom vs. less freedom. It is a matter of competing freedoms.

A classic scale, as in the scales often held by Lady Justice, shows two sides. The heavier has a healthcare provider’s stethoscope resting upon it.
For what it is worth, my position is that freedom to access health care via increased options is far more important than freedom to spend that portion of money on other goods, especially when ACA measures such as subsidies mitigate the burden imposed upon individuals by that mandate to have health insurance. If we are going to continue to use a for-profit medical insurance market as the basis for health coverage in the U.S.—vs. single-payer or co-op systems such as the UK and Germany respectively use—then the risk pool, and whether there is a commercially viable gap between premium revenues and actual payments for care, will dominate everything. To ensure that gap exists, we need many more people to pay premiums in order to make more care available and to cover persons with pre-existing conditions. Some folks will have to give up a little leeway on how they spend their money in order to make cheaper and better coverage available to all. Some freedoms are weightier than others.
