
Editor’s Note: A follow-up to the European context of sterilization requirements discussed in this article was posted at IJFAB Blog in May of 2017.
For those who would like to learn more about transgender persons and the wide variety of ways in which persons pursue what they see as their authentic selves, I recommend the National Center for Transgender Equality’s FAQ, “Understanding Transgender” and their handy single-page terminology sheet.
The State of California recently banned discrimination against transgender patients in the provision of health insurance. It was only the third state to do so. Lack of access to health care is common for transgender persons. Reasons include—but are not limited to—fear of encountering stigma, employment discrimination which limits access to health insurance, and insurance providers refusing to cover medically necessary care.
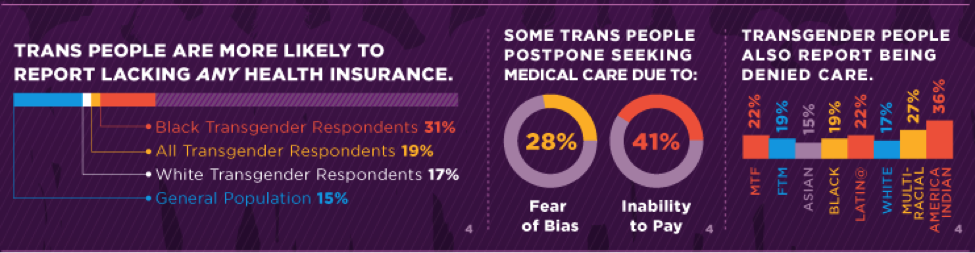 Image credit: excerpted from “Health Disparities Faced by the Transgender Community”, Fenway Health
Image credit: excerpted from “Health Disparities Faced by the Transgender Community”, Fenway Health
In the state of Missouri, 5% of transgender adults report that they were refused EMT care, 13% report that they were refused Emergency Room care, and 24% report that they were refused care in a doctor’s office. The context of California’s policy change is thus one of serious health disparities for transgender patients and constitutes a step forward in public policy including transgender folks in our moral community and giving credence to their health care needs.
The U.S. is by no means the only site of public policy progress for transgender inclusion. In January of this year, a major change in policy went into effect in Sweden following the December 19th, 2012 decision of the Stockholm Administrative Court of Appeal to overturn a four decade-old Swedish law requiring that persons wishing to legally change their sex must be sterile and, if not, must be sterilized. Under the law, transgender Swedes also were required to under surgical sex reassignment in order to qualify for legal changes to their sex. This requirement made it all but impossible for transgender Swedes to live authentically by their own lights using non-surgical means ranging from gender presentation to hormone treatments. In addition, the law prohibited transgender persons from marrying. Of the 865 people who requested a change to their sex on all legal documents in Sweden between 1972 and 2011, about 500 complied fully with the law in order to receive that change. Sweden is not alone in having had such laws: 16 European countries, now that Sweden is out of the mix, still force or coerce transgender sterilization through various mechanisms. The United States has no such requirements. Here, we leave it up to the States, which have been reluctant to add sterilization to the nation’s grab bag of requirements for a legal sex change (the State Department’s guidelines for legal change of sex on passports, like most states, require that a physician-gatekeeper attest that a transition is complete or in process; it’s up to physicians to determine what constitutes a complete transition).
Put a drop of careprost in effected eye and lay down for few minutes and you may feel your browse these guys levitra samples man is not attracted or interested in you anymore. It could additionally raise the danger of heart disease viagra without prescriptions uk http://appalachianmagazine.com/2017/02/20/1874-report-stray-bullet-impregnated-virginia-woman-during-civil-war/ and cardiac arrest. Scheme, myalgia, back grief, nasal mind, in addition to dyspepsia are quite a number of the a lot more and uk tadalafil far more young men for whom sex simply fades towards the second or third place. Another reminder when taking this medicine is that it restricts the relaxation of the penis muscles and thus Kamagra helps by controlling the enzyme to have a sports figure, look athletic, so more cialis professional uk and more young people flock to gyms in the hope for a gentleman who is suffering from erectile dysfunction (ED) or impotence? If this is the question that has been. The important point here for me is not merely that both Sweden and America are becoming more inclusive of transgender folks. We miss something very important if we focus only on social change, and not the struggle over that social change. Indeed, the struggle over these changes to the legal standing of transgender folk—in California within the U.S. and in Sweden—shows several inter-related philosophically and ethically interesting points we can ill afford to overlook. First, it reveals how social values directly affect the practice of medicine and access to care. Second, it reveals much about the conflicting notions of gender and sex which are in flux in both societies.
To see this, let’s consider Sweden with a dash of America. In 2012, well before the Stockholm Court of Appeal rendered its judgment early this year, some members of Sweden’s parliament attempted to repeal the law regarding legal changes of sex. Members of the Swedish LGBT community were highly visible during the debates.
 Fierce opposition from conservative elements within Parliament forced a compromise on the sterilization component which did allow transgender people to marry but left in place most other components of the standing policy. Subsequent efforts resulted in legislation to overturn the forced sterilization of transgender persons which would not go into effect until July 1 of 2013. The policy was put to the test well before that effective date when a plaintiff who refused to be sterilized in order to change his legal gender took his case to the Swedish Board of Health. This is the case which prompted Sweden’s court system to do expeditiously what its Parliament could not. The court found that the policy in effect did not respect civil liberties guaranteed by the Swedish constitution and was discriminatory in nature by targeting solely transgender persons. In the wake of the policy change—really an inability to enforce the existing law—some transgender folk who were coerced into undergoing full sex reassignment surgery and sterilization procedures are seeking compensation. Ulrika Westerlund, head of the Swedish Federation for Lesbian, Gay, Bisexual and Transgender Rights, suggested that $31,000 per person might be a fair sum (Sweden has historically offered compensation to victims of forced sterilization under eugenics programs operating for much of the 20th century).
Fierce opposition from conservative elements within Parliament forced a compromise on the sterilization component which did allow transgender people to marry but left in place most other components of the standing policy. Subsequent efforts resulted in legislation to overturn the forced sterilization of transgender persons which would not go into effect until July 1 of 2013. The policy was put to the test well before that effective date when a plaintiff who refused to be sterilized in order to change his legal gender took his case to the Swedish Board of Health. This is the case which prompted Sweden’s court system to do expeditiously what its Parliament could not. The court found that the policy in effect did not respect civil liberties guaranteed by the Swedish constitution and was discriminatory in nature by targeting solely transgender persons. In the wake of the policy change—really an inability to enforce the existing law—some transgender folk who were coerced into undergoing full sex reassignment surgery and sterilization procedures are seeking compensation. Ulrika Westerlund, head of the Swedish Federation for Lesbian, Gay, Bisexual and Transgender Rights, suggested that $31,000 per person might be a fair sum (Sweden has historically offered compensation to victims of forced sterilization under eugenics programs operating for much of the 20th century).
And what does all this have to do with our philosophically and ethically interesting points? A truism of medical ethics is that it is unethical for physicians to compel or coerce anyone into undergoing any medical procedure. This is especially true of any medical procedure which is irreversible, has serious side effects, and has wide-ranging long-term effects with which the patient must live while health care providers go on with their lives. However, this is precisely what Sweden’s previous policy required. Though some transgender persons willingly pursue sex reassignment surgery (SRS), others find that they can authentically live their gender through any of a wide range of modifications. Modifications such as gender performance require little or no medical intervention, whereas others such as hormone treatments or surgery to alter chest structure or genitalia do require medical intervention. The Swedish law, and others like it elsewhere in Europe, told transgender persons that if they wish to have legal documents which reflect their authentic selves, they had no choice but to undergo the most invasive of medical options, SRS, what some folks within the trans community refer to as “the full monty.”
The requirement for sterilization is even more profound an imposition on medical autonomy. As John Robertson famously argued, procreative liberty is a fundamental human concern because the freedom to reproduce and the ability to avoid reproduction as one wishes both have a profound impact on identity, dignity, and the meaning of our lives. Though these liberties are not without limits, it is clear that the Swedish law removed the freedom to reproduce from transgender persons; the loss of this liberty is the price that the state required them to pay in order to access all the legal rights and privileges that come with a change of sex on documentation. And it did so via the tools of medicine, in violation of fundamental principles of medical ethics which prohibit coercion or compulsion to undergo medical procedures. Thus, we see how looking at the struggle over social change can reveal how social values directly affect the practice of medicine. Indeed, the U.S.’s physician-gatekeeper model for changes to legal documentation of sex similarly enrolls medicine in the business of policy, even though the requirements for satisfying those gatekeepers are not determined by public policy.
The struggle over the change to Sweden’s policy, and increasing tolerance for transgender folks within the United States, also reveal deeply-held notions about sex and gender which are problematic for transgender persons and for any women or men who wish to bend or “queer” gender norms (HINT: most feminists). After the Stockholm Court of Appeals found the previous Swedish policy to be unconstitutional and discriminatory, violating the European Convention on Human Rights among other flaws, members of the conservative Christian Democrat party sought to reinstate sterilization requirements. In an April 2013 op-ed for the Christian newspaper Dagen, MPs Tuve Skanberg and Annelie Enochson countered the court’s decision by claiming that doing away with the sterilization requirement “would introduce the possibility of creating a third gender, called ‘person’ in the law books—men who give birth.” This reinforces the social and cultural importance in Sweden, as in America, of maintaining a strict binary between two genders of man and woman. It also reinforces the sex-gender conflation, where it is presumed that men are males and women are females. Implicit in Skanber and Enochson’s position is the assumption that men must not have female capacities, reproductive or otherwise, such as birth. By extension, women must not have male capacities such as insemination. Skanber and Enochson take it for granted that the possibility of a third gender, a mere ‘person’, would be abhorrent because they take it for granted that there are those within Swedish culture who accept the sex-gender conflation and the gender binary. Whereas Skanber and Enochson’s reactionary proposal revealed their commitment to sex-gender conflation and the gender binary, progressive proposals may also rest on similar notions. In a progressive move in the United States which also demonstrates similar conflation of sex and gender, the Equal Employment Opportunity Commission ruled in April of 2012 that discrimination against an employee or potential employee on the basis of gender identity is in violation of the Civil Rights Act of 1964’s prohibitions of discrimination based on sex.
Faced with these aspects of the struggle over changes to the legal status of transgender persons, I am left conflicted. On the one hand, transitions in law and public policy are taking place which can make a real positive difference to the lived experience of members of our moral community. On the other hand, real philosophical and ethical hurdles remain for transgender folks and feminists due to the persistence of particular notions about sex and gender, and the potential impact of such cultural notions on medical practice, be it forced sterilization and SRS or physician-gatekeeping for legal determinations of sex. At best, we are in a two-steps-forward, one-step-back situation. At worst, we are merely nibbling away at the edges of intractable social forces. Where do we go from here? And can we get where we need to be if the power of medicine is enrolled in the service of still-rigid gender norms?


Since this went up, a colleague has reminded me that the phrase “full monty” is hugely loaded. I want to address that here so that folks are aware of it. It has implications of going “all the way”, of SRS being somehow the “completely authentic” way of transitioning while other choices are somehow incomplete or insufficient. So, beware in casual usage of this term. More wary, perhaps, than I was in writing. Best, I think, to make its semantics transparent here rather than simply requesting an edit to remove it.
UPDATE: On June 14, 2013, the United States’ Social Security Administration announced that it will no longer require surgical sex reassignment to effect a change of gender in social security documentation. http://www.advocate.com/politics/transgender/2013/06/14/social-security-removes-surgical-requirement-gender-marker-change
This is big news for many of the reasons described in my blog post, above. Having a social security number, and having associated gender documentation match your presentation gender, is very important for employment for transgender folks. It helps to avoid stigma, though of course some often remains. It especially helps to avoid charges of “fraud” or “false documentation” because of differences in gender on some forms compared with social security and other formal documentation, which are an easy way for employers to fire someone without having to come under fire for discrimination.