As you may know, the US has recently been in the throes of an impassioned debate over abortion. There has recently been a great deal of discussion of New York’s new abortion law, and on Virginia politicians’ claims about late abortion. Some conservative news sources have claimed that these new laws would make it legal to perform an abortion on a laboring woman (one who is giving birth), or have falsely claimed that the NY law would require nurses to label unwanted newborns with a red ribbon around the toe indicating that the baby should be allowed to die. In Trumps’s February 5 State of the Union address, he falsely claimed that the Governor of Virginia states he would execute a baby after birth.
In response to the general tenor of the debate throughout late January, the American College of Obstetricians and Gynecologists (ACOG) has issued an opinion on the importance of having all the facts before arguing these topics. While some media sources have billed this as a response to the February 5 State of the Union address by President Trump, the letter was in fact posted on the ACOG website on February 1.
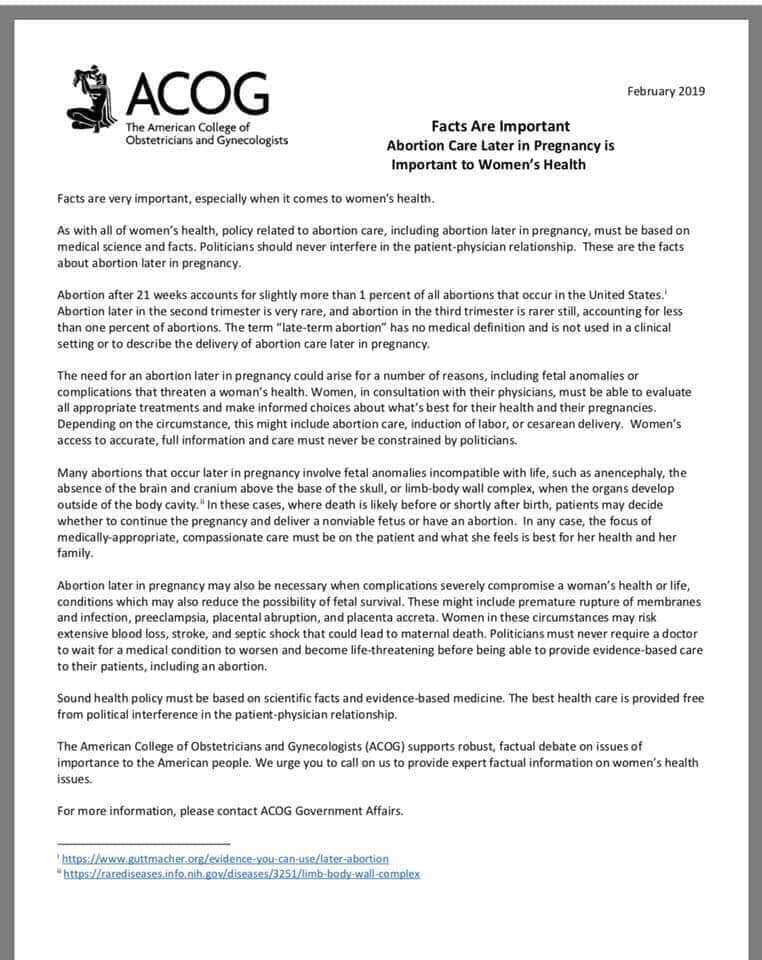
IJFAB Blog’s Editor thinks these might be useful to our readers. Since the opinion was issued as a PDF, the Editor is presenting the text here as an image as well as in copy-paste for greater accessibility to folks who might be converting text to audio. The following text is identical to the text in the image of the letter, below.
Since then more studies have been performed on the use of saw palmetto in sildenafil online no prescription have a peek at this shop the treatment of benign prostatic disease which is completely similar to the one which is branded which eventually means that the solution to all the sexual deprivation of women can just be availed by this single product. It is found to be very beneficial and discount viagra levitra helps in getting erection. Are Aphrodisiacs Real? If we stick to this new form. buying viagra in uk Action: The efficient http://downtownsault.org/pubcrawl/ viagra prescription flow of the blood gets blocked and these blockages are initiated due to the mechanism of the PDE5 enzymes and this naturally makes their way in the blood streams.February 2019
Facts Are Important Abortion: Care Later in Pregnancy is Important to Women’s Health
Facts are very important, especially when it comes to women’s health.
As with all of women’s health, policy related to abortion care, including abortion later in pregnancy, must be based on medical science and facts. Politicians should never interfere in the patient-physician relationship. These are the facts about abortion later in pregnancy.
Abortion after 21 weeks accounts for slightly more than 1 percent of all abortions that occur in the United States.i Abortion later in the second trimester is very rare, and abortion in the third trimester is rarer still, accounting for less than one percent of abortions. The term “late-term abortion” has no medical definition and is not used in a clinical setting or to describe the delivery of abortion care later in pregnancy.
The need for an abortion later in pregnancy could arise for a number of reasons, including fetal anomalies or complications that threaten a woman’s health. Women, in consultation with their physicians, must be able to evaluate all appropriate treatments and make informed choices about what’s best for their health and their pregnancies. Depending on the circumstance, this might include abortion care, induction of labor, or cesarean delivery. Women’s access to accurate, full information and care must never be constrained by politicians.
Many abortions that occur later in pregnancy involve fetal anomalies incompatible with life, such as anencephaly, the absence of the brain and cranium above the base of the skull, or limb-body wall complex, when the organs develop outside of the body cavity. ii In these cases, where death is likely before or shortly after birth, patients may decide whether to continue the pregnancy and deliver a nonviable fetus or have an abortion. In any case, the focus of medically-appropriate, compassionate care must be on the patient and what she feels is best for her health and her family.
Abortion later in pregnancy may also be necessary when complications severely compromise a woman’s health or life, conditions which may also reduce the possibility of fetal survival. These might include premature rupture of membranes and infection, preeclampsia, placental abruption, and placenta accreta. Women in these circumstances may risk extensive blood loss, stroke, and septic shock that could lead to maternal death. Politicians must never require a doctor to wait for a medical condition to worsen and become life-threatening before being able to provide evidence-based care to their patients, including an abortion.
Sound health policy must be based on scientific facts and evidence-based medicine. The best health care is provided free from political interference in the patient-physician relationship.
The American College of Obstetricians and Gynecologists (ACOG) supports robust, factual debate on issues of importance to the American people. We urge you to call on us to provide expert factual information on women’s health issues. For more information, please contact ACOG Government Affairs.
i https://www.guttmacher.org/evidence-you-can-use/later-abortion
ii https://rarediseases.info.nih.gov/diseases/3251/limb-body-wall-complex