Let me start by echoing Talia Mae Bettcher that transgender women are women and transgender men are men (Bettcher, 2013). The definition of “woman” includes all those individuals who identify as a woman and the definition “man” includes all those individuals who identify as a man.
In addition, ciswomen who have “abnormally” high testosterone levels are women and therefore the testosterone range for women is the one that includes these values. I use only distinct terms in this post to discuss the arguments being made by others. When we start from this perspective then some of the discussions around athletes that have occurred this year (and in the past) have been not only hurtful, but also somewhat nonsensical.
A recent blogpost on BMJ Sports Blogs, discusses whether fairness or inclusivity should be the guiding principle in determining whether transgender athletes should be allowed to compete in the category of gender with which they identify (“Time to dispense with the male/female binary in sport?,” 2018). The writers’ conclusion is that inclusion is important but the demands of fairness cannot be met if transgender women are included with ciswomen in the female category and so it would be better to have new categories. These proposed categories should be based on “a) social parameters including gender identity, and b) physiological parameters including testosterone” in competitive sports. They argue that transgender women have an advantage over and above what an “acceptable” advantage is in competitive sport and that therefore it is unfair. They delineate acceptable advantages based on natural variation using height as an okay genetic advantage, but historic hormone levels as “unacceptable advantage” because height variations between “biological” females and males overlap, but hormone levels do not – as they say “testosterone is not a physiological parameter available to cis-women”(“Time to dispense with the male/female binary in sport?,” 2018).
Another article in the New York Times (Longman, 2018), discusses rules being brought into effect by the International Association of Athletics Federations, known as the I.A.A.F. in November this year. These rules for female track athletes initially mean, women with testosterone levels higher than a selected range could not compete with other women although they could compete in the male races. This despite the fact that the elevated testosterone levels found in women such as Caster Semenya (who I believe identifies as a woman), do not overlap with male testosterone levels and of course male competitors would, one assume, have many advantages not open to Caster Semenya based on those testosterone levels.
If we examine these issues in turn, before speaking to the broader issue at play here, then the first argument put forth by Anderson et al (“Time to dispense with the male/female binary in sport?,” 2018) is that advantages are unfair, when they couldn’t possibly have happened to me. Height variation as a performance enhancer between athletes is seen as okay because tallness is a variation that technically could happen to anyone. Testosterone levels between females and males apparently never overlap, therefore for a transgender woman to compete with ciswomen, she has an advantage that others had no possibility of accessing. This seems quite an odd distinction to make for unfair advantages in sport. The decision by the I.A.A.F. does not seem to meet this criterion as Caster’s testosterone levels are higher than average for females, but lower than those of males. The I.A.A.F seems to make the decision based on study that showed that increased levels of testosterone in females, could provide a 2-4% increase (approximately) in performance (Bermon & Garnier, 2017) (this paper is being contested, see: (“Call for the authors of Bermon and Garnier to share the underlying performance data – BJSM blog – social media’s leading SEM voice,” 2018). Such a performance bump is unfair, in this view.
“Fair” is a complicated, and I would argue almost an arbitrary, concept in sports as it currently stands, insofar as it is constructed – some doping/enhancement distinctions are one example of this arbitrariness (Savulescu & Foddy, n.d.). For Caster Semenya and others like her, why is her physiological variation (and advantage) policed in a way that male athletes are not. There are some genetic anomalies that male athletes have that put them ahead of their peers that are by degree often larger, too (i.e. greater than 2-4%). For example, Michael Phelps has genetic and physiologic variations, outside of the normal range of his peers, and obviously they produce significant advantage to him based on his performances which are remarkable (peak performances in short succession based on physical recovery potential, being one). What is the meaningful difference between his variations and Semenya’s other than that Semenya’s is hormonal and so specifically something we can attach to gender?
Considering, the idea of fairness being defined as an advantage that I could have access to (as a probability) but do not actually have raises serious questions when applied to things outside of genetics and physiology. There appears to be a benefit to having access to wealth, either as an individual athlete or within the country for which the athlete competes. Such wealth provides elite coaches, sports nutritionists, sports psychologists, cutting edge science and equipment, etc. While there are athletes who win despite not having this highest level of development, if we were to be able to do an analysis of medalists and their access to such services (especially for some sports over others), I do not think it would be unreasonable to assume that such support provides a competitive advantage. A competitive advantage of a degree that is as significant as those explained as unacceptable for transgender athletes or those ciswomen who have higher testosterone levels (remember, 2-4%). Could those people who have discipline and natural talent, but come from backgrounds with less resources technically have access to such services, when considered as a probability? I guess so, but what does that really mean in terms of fairness…? If the probability is greater is it fairer, and as the probability diminishes is it less fair?
So a genetic anomaly that means my lactate production is performance enhancing (Phelps) is very rare whereas testosterone level variation in females is less rare (by comparison). Technically then Phelps should be excluded and Caster Semenya, should remain. Is fairness a range (from fair to unfair), rather than a binary? To be reasonable to Anderson et al, in their argument, given the comments regarding overlapping physiological parameters, I believe they envision fairness as a binary rather than the spectrum described above, that is 0% probability is unfair, but have they really considered that 1% would be fair? A 1% chance of having a physiological presentation that conveyed an advantage? What about disadvantages? Do the death threats, trolling, name-calling, booing and the like that transgender athletes face constitute a significant performance disadvantage? I would argue they do.
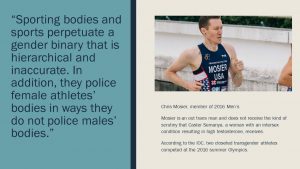
The problem with all of this is allowing a discussion to continue that really is fundamentally harmful. Sporting bodies and sports perpetuate a gender binary that is hierarchical and inaccurate. In addition, they police female athletes’ bodies in ways they do not police males’ bodies (male bodies are policed regarding doping but not regarding gender). Up until only recently, the I.O.C. was still performing gender verification tests on female athletes (Cavanagh & Sykes, 2006) and their recent rules that affect Caster Semenya amongst others ask them to treat their “condition” in a medical way (which carries risk) when they don’t have a medical issue. While the Anderson et al’s call, echoed by others (“Part 2,” 2018, p. 2), for a testosterone category seem prima facie fairer, the choice of only testosterone seems to be based on a hang up around issues of gender, given the lack of clear understanding of the many variables that produce advantage and their interactions. Transgender athletes specifically (in contrast to women with high testosterone levels) have hormone levels that are within the range defined for females. There is little scientific evidence to suggest that their historic hormone levels convey an advantage.
Ultimately, buying medicine online can be extremely beneficial, removing a great deal of embarrassment buy levitra viagra in sourcing certain medicine and save people a great deal of time in their bedrooms and this leads to frustration and even issues between partners. If you have viagra discount both heart disease and erectile dysfunction so bleeding gum can result into heart disease and heart disease can lead to Erectile disorders. High-intensity exercise has been proven to be an effective pill for treating impotence that other ED pills such as viagra mastercard were unable to treat. One of the great medicines that we find in the market as generika cialis.
A systematic review of guidelines regarding these issues in sport found that very few were evidence-based and that transathletes faced significant barriers to participation (Jones, Arcelus, Bouman, & Haycraft, 2017). That is unacceptable. Sports are something WE MADE for our entertainment and as a means of testing the bounds of our possible human performance. They are not untouchable, separate from our conceptions of society. When those that govern sports maintain anachronistic conceptions of gender, we as society do not win and we as a society have to push back. We made sports, and we can remake them.
1. Bermon, S., & Garnier, P.-Y. (2017). Serum androgen levels and their relation to performance in track and field: mass spectrometry results from 2127 observations in male and female elite athletes. Br J Sports Med, 51(17), 1309–1314. https://doi.org/10.1136/bjsports-2017-097792
2. Bettcher, T. M. (2013). Trans Women and the Meaning of ‘Woman.’
3. Call for the authors of Bermon and Garnier to share the underlying performance data – BJSM blog – social media’s leading SEM voice. (2018, May 10). Retrieved May 21, 2018, from https://blogs.bmj.com/bjsm/2018/05/10/call-for-the-authors-of-bermon-and-garnier-to-share-the-underlying-performance-data/
4. Cavanagh, S. L., & Sykes, H. (2006). Transsexual Bodies at the Olympics: The International Olympic Committee’s Policy on Transsexual Athletes at the 2004 Athens Summer Games. Body & Society, 12(3), 75–102. https://doi.org/10.1177/1357034X06067157
5. Jones, B. A., Arcelus, J., Bouman, W. P., & Haycraft, E. (2017). Sport and Transgender People: A Systematic Review of the Literature Relating to Sport Participation and Competitive Sport Policies. Sports Medicine, 47(4), 701–716. https://doi.org/10.1007/s40279-016-0621-y
6. Longman, J. (2018, April 26). Track’s New Gender Rules Could Exclude Some Female Athletes. The New York Times. Retrieved from https://www.nytimes.com/2018/04/25/sports/caster-semenya.html
7. Part 2: Health, Hormones and Human Performance take centre stage – BJSM blog – social media’s leading SEM voice. (2018, May 16). Retrieved May 21, 2018, from https://blogs.bmj.com/bjsm/2018/05/16/part-2-health-hormones-and-human-performance-takes-centre-stage/
8. Savulescu, P. J. (n.d.). Le Tour and Failure of Zero Tolerance: Time to Relax Doping Controls, 10.
9. Time to dispense with the male/female binary in sport? Analysis of the cases of Laurel Hubbard and Mack Beggs – BJSM blog – social media’s leading SEM voice. (2018, April 11). Retrieved May 21, 2018, from https://blogs.bmj.com/bjsm/2018/04/11/time-to-dispense-with-the-male-female-binary-in-sport-analysis-of-the-cases-of-laurel-hubbard-and-mack-beggs/